Pancreas
👩⚕️ Work your way through this list of MCQs. Hover over each option for the answers and explanations.
Which enzyme is responsible for autodigestion in acute pancreatitis?
- ((Lipase::Causes fat necrosis but is activated downstream))
- ((Elastase::Causes vascular damage and haemorrhage but not the initiating enzyme))
- ((Trypsin::☑️ Premature activation of trypsinogen to trypsin activates other pancreatic enzymes causing autodigestion))
- ((Amylase::Marker enzyme; does not cause tissue destruction))
- ((None of the above::Incorrect — trypsin is the key initiating enzyme))
💡 Normally, inactive trypsinogen is secreted by the pancreas and activated to trypsin in the duodenum by enterokinase. In acute pancreatitis, trypsinogen is activated prematurely into trypsin within the pancreas. Trypsin then activates other digestive enzymes (lipase, elastase, and phospholipase A2), initiating autodigestion and tissue damage.
A man is admitted with haemorrhagic pancreatitis. Which enzyme causes haemorrhagic pancreatitis?
- ((Lipase::Causes fat necrosis, not haemorrhage))
- ((Amylase::Diagnostic marker only))
- ((Pepsin::Gastric enzyme, not involved in pancreatitis))
- ((Trypsin::Activates other enzymes but does not directly cause haemorrhage))
- ((Elastase::☑️ Elastase causes haemorrhage by destroying vessel walls))
💡 Tryspin is the initiator. Elastase destroys blood vessels, causing haemorrhage in the pancreas.
Enterokinase
↓ (fast)
Trypsinogen ─────────→ Trypsin + TAP
▲ │
│ │
└──────── Autoactivation ─┘
Trypsin then activates:
Chymotrypsinogen ─────────→ Chymotrypsin
Proelastase ─────────→ Elastase
Kallikreinogen ─────────→ Kallikrein
Procarboxypeptidase A ─────────→ Carboxypeptidase A
Procarboxypeptidase B ─────────→ Carboxypeptidase B
Prophospholipase A2 ─────────→ Phospholipase A2
Procolipase ─────────→ ColipaseA male is diagnosed with chronic pancreatitis. He reports that his stool sticks to the commode and will not flush away. Loss of which enzyme is most likely responsible for this problem?
- ((Lipase::☑️ Fat malabsorption in chronic pancreatitis leads to steatorrhoea; lipase deficiency causes greasy, difficult-to-flush stools))
- ((Amylase::Carbohydrate digestion; deficiency does not cause fatty stools))
- ((Trypsin::Protein digestion; deficiency causes protein malabsorption, not steatorrhoea))
- ((Elastase::Protease for protein breakdown; not responsible for fat digestion))
💡 In pancreatitis, lipase is the first and most affected, and deficiency leads to undigested fat with floating, sticky stools.
A 50-year-old woman presents with a history of right upper quadrant pain and jaundice which is progressive and unremitting. She reports that her urine was dark in colour and that her stools are offensive and difficult to flush. By examination she has a palpable mass in the right upper quadrant region. Diagnosis?
- ((Chronic calculous cholecystitis::Typically recurrent RUQ pain; does not cause progressive jaundice with pale offensive stools))
- ((Primary biliary cirrhosis::Causes cholestatic pruritus but not a palpable RUQ mass))
- ((Gallbladder abscess::Would present with acute sepsis and RUQ tenderness rather than progressive unremitting jaundice))
- ((Carcinoma head of pancreas::☑️ Progressive painless obstructive jaundice with dark urine, pale offensive stools; palpable RUQ mass from distended gallbladder))
- ((CBD stones::Usually intermittent jaundice/colic; less likely to cause palpable gallbladder))
💡 Courvoisier’s sign, painless jaundice with a palpable gallbladder, indicates a diagnosis of pancreatic carcinoma
In a case of chronic pancreatitis, what is the first non-invasive test to be done?
- ((Lipase::Lipase typically normal or only mildly raised in chronic pancreatitis; not useful for diagnosis))
- ((Amylase::Amylase often normal in chronic disease and not sensitive for exocrine insufficiency))
- ((Faecal elastase::☑️ Faecal elastase is a non-invasive stool test assessing exocrine pancreatic insufficiency))
- ((Serum trypsin::Serum trypsin less sensitive and not routinely used as first-line non-invasive test))
A patient presents with an acute abdomen. Investigations reveal a serum amylase of 110 U/L, calcium of 2.4 mmol/L, and normal liver function tests. Diagnosis?
- ((Acute intermittent porphyria::☑️ Severe abdominal pain with normal amylase and LFTs; metabolic cause rather than surgical pancreatitis))
- ((Perforation::Would cause peritonism; amylase not typically elevated))
- ((Pancreatitis::Amylase not ≥3× upper limit and calcium normal; does not support diagnosis))
- ((Lead poisoning::Causes colicky abdominal pain and neuropathy but not acute surgical abdomen picture))
💡 Acute intermittent porphyria is an autosomal dominant disorder of heme synthesis (porphobilinogen deaminase deficiency). It causes severe abdominal pain, neuropathy, psychiatric symptoms, and dark urine precipitated by drugs, alcohol, fasting, or infection, despite normal imaging and routine labs. It is treated with IV hemin and glucose.
An 18-year-old woman recently started the combined oral contraceptive pill and now presents with acute abdominal pain, vomiting, and muscle weakness. Her pulse rate is 86 bpm, blood pressure 160/85. Investigations show amylase 110L, calcium 2.41, glucose 5, triglycerides 1.5. Other LFTs are within normal range. Diagnosis?
- ((Acute intermittent porphyria::☑️ Fits the picture: Young woman, precipitated by drugs e.g. OCP, recurrent severe abdominal pain, neuro symptoms e.g. weakness, hypertension; labs not diagnostic for pancreatitis/diabetes))
- ((Diabetic ketoacidosis::Normal glucose, no ketones or acidosis described))
- ((Hypoparathyroidism::Calcium is normal, no tetany or low Ca features))
- ((Mumps::Would cause parotitis ± pancreatitis, but presentation is not suggestive))
- ((Pancreatitis::In true pancreatitis, amylase usually >3× upper limit))
A patient with epigastric pain has an amylase 900, normal GGT and ALP, and a slightly raised bilirubin. Diagnosis?
- ((Alcoholic pancreatitis::☑️ Significantly elevated amylase indicates acute pancreatitis; normal ALP/GGT suggests non-obstructive cause))
- ((Choledocholithiasis::Would produce cholestatic pattern with raised ALP and GGT))
- ((Biliary colic::Does not cause marked amylase elevation))
- ((Acute cholecystitis::May raise inflammatory markers but not amylase to this degree))
A patient with acute pancreatitis is managed conservatively. A repeat CT after 4 days shows diffuse peripancreatic fluid and non-enhancing pancreatic tissue. Diagnosis?
- ((Pseudocyst::Develops >4 weeks after pancreatitis and has a well-defined wall))
- ((Pancreatic abscess::Would show rim-enhancing collection with systemic infective features))
- ((Pancreatic necrosis::☑️ Non-enhancing pancreatic tissue on contrast CT represents necrosis))
- ((Interstitial oedematous pancreatitis::Pancreas enhances on contrast CT; no areas of non-enhancement))
💡 Pancreatic necrosis shows up as non-enhancing areas of the pancreas due to ischaemia. It may later lead to infected necrosis or pseudocyst formation.
A patient with chronic pancreatitis presents with intractable back pain not responding to medical treatment. Management?
- ((NSAIDs::May be tried initially but often ineffective for chronic visceral pancreatic pain))
- ((Coeliac plexus block::☑️ Effective for intractable visceral pain in chronic pancreatitis))
- ((Long-term opioids::Associated with tolerance and dependence; not preferred definitive solution))
- ((Pancreatic enzyme supplementation::Improves malabsorption but does not relieve severe neuropathic pain))
💡 Pain in chronic pancreatitis is often deep, visceral, and radiating to the back, due to inflammation, fibrosis, and nerve involvement. Coeliac plexus block (or neurolysis) is especially useful for severe, refractory pain, reducing opioid needs and improving quality of life.
A woman has jaundice and liver metastasis secondary to a pancreatic head carcinoma. Management?
- ((Endoscopic biliary stent (ERCP)::☑️ Palliative biliary decompression to relieve obstructive jaundice in metastatic disease))
- ((Whipple procedure::Not indicated in presence of liver metastases; disease is unresectable))
- ((Curative radiotherapy::Not curative in metastatic pancreatic cancer))
- ((Observation only::Obstructive jaundice requires palliation to prevent cholangitis and improve symptoms))
A patient presents hypoglycemia, confusion, sweating, and relief after eating. Blood tests show high insulin and high C-peptide levels. Diagnosis?
- ((Exogenous insulin administration::Exogenous insulin causes ↑ insulin with ↓ C-peptide))
- ((Insulinoma::☑️ Endogenous insulin overproduction causes ↑ insulin and ↑ C-peptide))
- ((Glucagonoma::Causes hyperglycaemia, not hypoglycaemia))
- ((Type 1 diabetes mellitus::Causes low or absent insulin and low C-peptide))xXx
💡 In insulinoma, an islet cell tumour of the pancreas, there is autonomous secretion of insulin, leading to hypoglycemia with ↑insulin and ↑ C-peptide. Factitious hypoglycaemia would show ↑insulin but suppressed ↓ C-peptide.
A teacher who frequently misses her morning meal swears and sweats in the morning, and her behaviour returns to normal after eating. What is the diagnosis?
- ((Insulinoma::☑️ Fasting hypoglycaemia with sweating and behavioural change that improves after eating — Whipple’s triad))
- ((Reactive hypoglycaemia::Occurs post-prandially, not after missed meals))
- ((Phaeochromocytoma::Causes episodic sweating and hypertension but not fasting hypoglycaemia relieved by food))
- ((Anxiety/panic attacks::May cause sweating but not true hypoglycaemia with resolution after meals))
A patient presents with episodes of fainting and sweating following exercise. She has a history of parathyroid disease. Diagnosis?
- ((Insulinoma::☑️ Hypoglycaemic episodes with sweating and syncope; association with MEN1 (parathyroid + pancreatic endocrine tumour)))
- ((Glucagonoma::Causes hyperglycaemia and necrolytic migratory erythema, not hypoglycaemia))
- ((VIPoma::Causes watery diarrhoea, hypokalaemia, achlorhydria (WDHA), not fainting from hypoglycaemia))
- ((Gastrinoma::Causes refractory peptic ulcers (Zollinger–Ellison), not hypoglycaemic episodes))
- ((None of the above::Incorrect — insulinoma fits the MEN1 context))
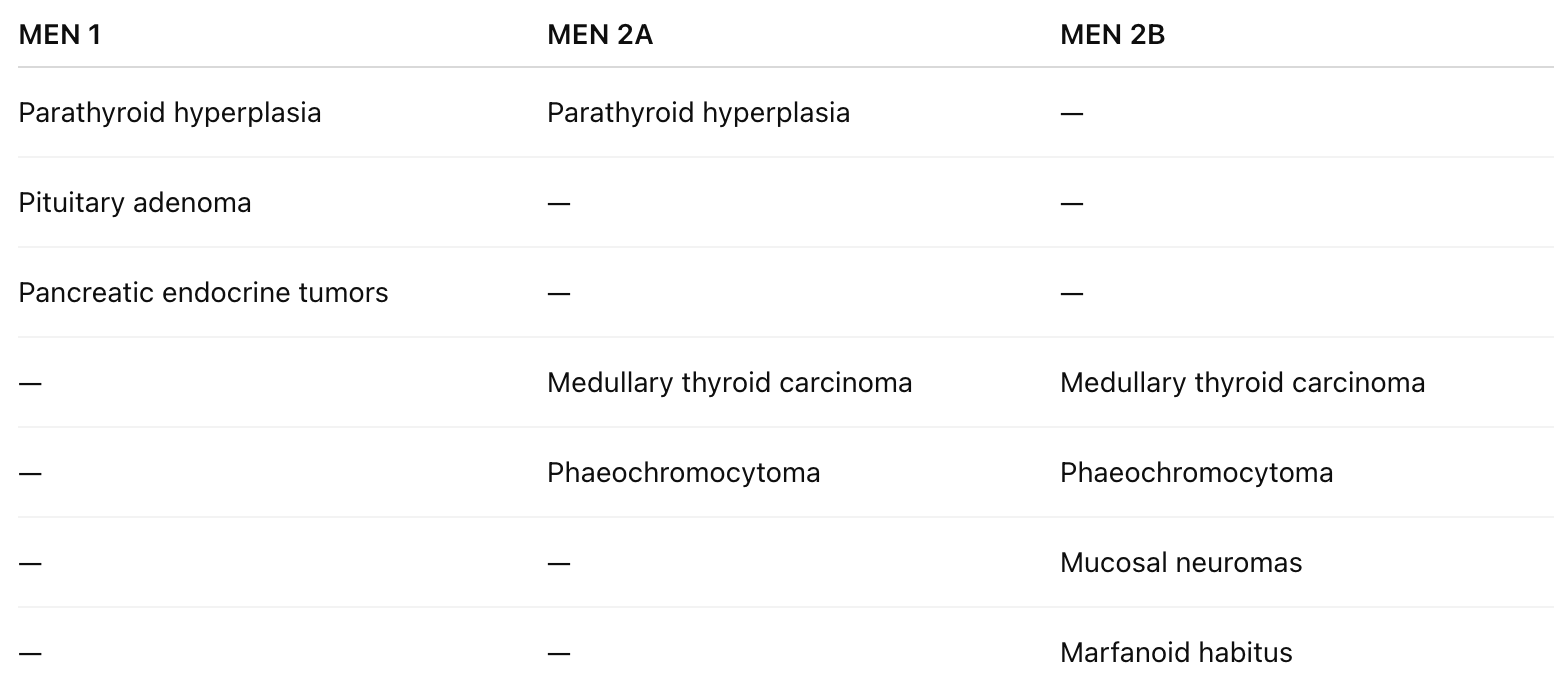
💡 Remember MEN1 syndrome?