Spleen
Which of the following statements about the spleen is true?
- ((Haemopoiesis in normal individual::In adults, haemopoiesis ceases after birth; extramedullary haemopoiesis occurs only in pathological states))
- ((Contains macrophages::☑️ The red pulp contains cords and sinusoids rich in macrophages responsible for filtration and removal of aged red cells))
- ((Primary lymphoid organ::Primary lymphoid organs are the thymus and bone marrow; the spleen is a secondary lymphoid organ))
- ((Contains medullary sinuses::Medullary sinuses are a feature of lymph nodes, not the spleen))
💡Lienorenal (Splenorenal) ligament VS Gastrosplenic ligament
- Lienorenal (Splenorenal) ligament
- Connects the spleen to the posterior abdominal wall, overlying the left kidney
- Contents of the lienorenal ligament:
- Splenic artery
- Splenic vein
- Tail of the pancreas
- Lymph nodes
- Gastrosplenic ligament
- Connects the spleen to the greater curvature of the stomach
- Contents of the gastrosplenic ligament:
- Short gastric veins, draining to the splenic vein
- Short gastric arteries, branches of the splenic artery
- Left gastroepiploic artery, another branches of the splenic artery
- Left gastroepiploic vein, another branches of the splenic artery
Which structure is at greatest risk during splenectomy?
- ((Adrenal gland::The left adrenal lies posteriorly and is not commonly injured during routine splenectomy))
- ((Diaphragm::Although adjacent superiorly, it is not the structure at greatest risk))
- ((Transverse colon::The splenic flexure is mobilised, but it is not the structure most at risk))
- ((Tail of the pancreas::☑️ The tail of the pancreas lies in the splenorenal ligament close to the splenic hilum and is at greatest risk of injury during splenectomy))
A patient underwent splenectomy after trauma. During the operation the surgeon was due to ligate the splenic artery. What is the structure most likely to be injured during this step?
- ((Tail of pancreas::☑️ The splenic artery runs along the superior border of the pancreas toward the splenic hilum; the tail of the pancreas lies close to the splenic vessels and is at greatest risk during ligation))
- ((Fundus of stomach::Related via the short gastric vessels, but not the structure most at risk during splenic artery ligation))
- ((Pancreatic duct::Although within the pancreas, it is not directly at risk unless the pancreatic tail is injured))
- ((Phrenicocolic ligament::Supports the spleen inferiorly but is not related to the splenic artery))
During ligation of the splenic hilum in splenectomy, which structure must be carefully avoided?
- ((Greater curvature of the stomach::Short gastric vessels are divided near this area, but the stomach itself is not the structure most at risk at the hilum))
- ((Left kidney::Lies posteriorly and is separated from the hilum by peritoneum and fascia))
- ((Splenic flexure of colon::Mobilised during splenectomy but not directly at risk during hilar ligation))
- ((Tail of pancreas::☑️ The tail of the pancreas lies within the splenorenal (lienorenal) ligament and is closely related to the splenic vessels at the hilum, making it highly vulnerable during ligation))
💡 During a splenectomy, the surgeon dissects at the splenic hilum to ligate the splenic vessels, which lie within the lienorenal (splenorenal) ligament, which is where the tail of the pancreas is located. Because of this close relationship, surgeons take care to avoid injuring the pancreatic tail during dissection; damage could result in a pancreatic fistula.
Which structure is liable for direct injury while ligating short gastric vessels in splenectomy?
- ((Tail of pancreas::The tail of the pancreas is at risk during hilar ligation, not during division of short gastric vessels))
- ((Greater curvature of stomach::The short gastric vessels run along the greater curvature but supply the fundus specifically))
- ((Fundus of stomach::☑️ The short gastric vessels run in the gastrosplenic ligament and supply the fundus, which is at risk during their ligation))
- ((Left kidney::Lies posteriorly and is not related to the gastrosplenic ligament))
💡 Splenectomy danger zones:
- Short gastric vessels → Fundus of stomach
- Splenic hilum → Tail of pancreas
- Splenorenal ligament → Tail of pancreas
- Splenic vessels → Tail of pancreas
During emergency splenectomy, it is essential to control bleeding from the splenic vessels. Where do these lie?
- ((Gastocolic ligament::Connects the stomach to the transverse colon; does not contain the splenic vessels))
- ((Greater omentum::Hangs from the greater curvature of the stomach; does not contain the splenic artery and vein))
- ((Lesser omentum::Contains the portal triad in the hepatoduodenal ligament, not the splenic vessels))
- ((Lienorenal ligament::☑️ Connects the spleen to the posterior abdominal wall and contains the splenic artery, splenic vein, and tail of the pancreas))
A surgeon is carrying out an elective splenectomy for congenital spherocytosis. Which structure will be divided in order to mobilise the spleen from the posterior abdominal wall?
- ((Gastrosplenic ligament::Connects the greater curvature of the stomach to the spleen and contains the short gastric vessels))
- ((Lesser omentum::Connects the stomach and duodenum to the liver; not involved in posterior splenic mobilisation))
- ((Phrenicocolic ligament::Supports the inferior pole of the spleen but does not attach it to the posterior abdominal wall))
- ((Lienorenal ligament::☑️ Connects the spleen to the posterior abdominal wall and contains the splenic vessels and tail of the pancreas; must be divided to mobilise the spleen))
Post-splenectomy, which blood component is affected first?
- ((Platelets causing thrombocytosis::☑️ The spleen normally sequesters platelets; after splenectomy, platelet count rises rapidly causing reactive thrombocytosis))
- ((Platelets causing thrombocytopenia::Splenectomy removes sequestration and destruction, so platelet count increases rather than decreases))
- ((Reticulocytes::May increase in haemolytic disorders, but not the earliest or primary change post-splenectomy))
- ((Granulocytes::White cell count may rise transiently, but the most immediate and marked change is thrombocytosis))
Which of the following parameters would be expected in a blood film after splenectomy for blunt trauma?
- ((High platelet count::☑️ The spleen normally sequesters platelets; following splenectomy there is reactive thrombocytosis, typically evident within days))
- ((High basophils::Not a characteristic early post-splenectomy finding))
- ((Neutrophilia::White cell count may rise transiently, but thrombocytosis is the most consistent early change))
- ((Lymphocytosis::Not the primary or earliest haematological change after splenectomy))
💡 The spleen normally removes and stores platelets. After splenectomy, this filtering function is lost, leading to platelet accumulation in circulation and transient thrombocytosis > 500,000/mm³ typically within days to a week after surgery. Persistent thrombocytosis may increase thrombotic risk, so patients may need antiplatelet therapy temporarily.
A child had a splenectomy. A week later, a peripheral blood film is sent. Which of the following is NOT expected?
- ((Low WBC count::☑️ White cell count typically increases after splenectomy due to loss of splenic sequestration))
- ((Target cells::Seen post-splenectomy due to altered red cell membrane processing))
- ((Pappenheimer bodies::Iron-containing inclusions normally removed by the spleen; seen after splenectomy))
- ((Heinz bodies::Denatured haemoglobin inclusions that may be seen because the spleen normally removes them))
💡 Blood film in hyposplenism:
- Blood counts increase
- Platelet, granulocyte, and reticulocyte count increase first
- Lymphocyte and monocyte counts take several weeks to increase
- Howell-Jolly bodies, due to absence of splenic filtration
- Pappenheimer bodies
- Poikilocytes (target cells)
- Siderocytes: Erythrocytes containing siderotic granules
- Heinz bodies
A patient had a splenectomy 2 years ago. In the normal spleen, macrophages are found mainly in which region?
- ((White pulp::Primarily contains lymphocytes arranged around central arterioles; not the main site of macrophages))
- ((Cortex::The spleen does not have a cortex; this is a feature of lymph nodes))
- ((Mantle zone::Part of the white pulp surrounding germinal centres; mainly contains B lymphocytes))
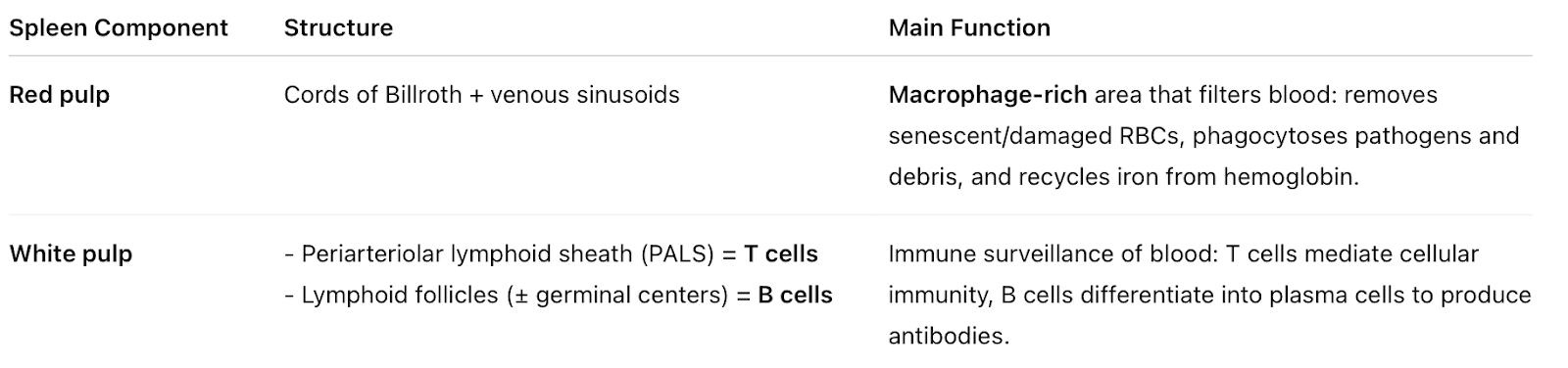
- ((Red pulp::☑️ The red pulp contains splenic cords (of Billroth) and sinusoids rich in macrophages responsible for removal of aged red cells and debris))
💡 Red pulp’s cords of Billroth and sinusoids house macrophages that remove old erythrocytes and pathogens. White pulp lymphoid follicles (germinal centers) and periarteriolar lymphoid are rich in B and T lymphocytes.
A tortuous vessel arising from the coeliac axis is identified during imaging. Which of the following does it supply?
- ((Pancreatic head::Supplied mainly by the superior and inferior pancreaticoduodenal arteries))
- ((Duodenum::Supplied by the superior and inferior pancreaticoduodenal arteries))
- ((Gastric fundus::☑️ The tortuous splenic artery (branch of the coeliac trunk) gives rise to short gastric arteries that supply the fundus of the stomach))
- ((Ascending colon::Supplied by branches of the superior mesenteric artery))
💡 The most characteristically tortuous branch of the coeliac trunk is the splenic artery, which takes a winding course along the superior border of the pancreas to reach the spleen. The splenic artery gives off short gastric arteries that supply the fundus of the stomach.
The inferior mesenteric vein most commonly drains into the:
- ((Superior mesenteric vein::The SMV joins the splenic vein to form the portal vein; the IMV does not usually drain directly into the SMV))
- ((Splenic vein::☑️ The inferior mesenteric vein most commonly drains into the splenic vein, which then joins the superior mesenteric vein to form the portal vein))
- ((Portal vein::The portal vein is formed by the union of the SMV and splenic vein; IMV usually drains before this point))
- ((Inferior vena cava::The IMV is part of the portal venous system, not the systemic venous system))
💡 IMV → splenic vein → joins SMV → portal vein.
A 50-year-old alcoholic woman with liver cirrhosis and platelet count < 50, splenomegaly present. What is the most common cause of thrombocytopenia?
- ((Ineffective production in bone marrow::Alcohol can suppress bone marrow, but this is not the most common cause in cirrhosis with splenomegaly))
- ((Platelet destruction in the liver::Platelets are not primarily destroyed in the liver in cirrhosis))
- ((Platelet destruction in the spleen::Immune destruction can occur, but this is not the main mechanism in portal hypertension))
- ((Platelet sequestration in the spleen::☑️ Portal hypertension leads to splenomegaly and hypersplenism, causing increased sequestration of platelets))
A 45-year-old man with established cirrhosis has splenomegaly and persistent thrombocytopenia. Bone marrow shows megakaryocyte hyperplasia. What is the most likely cause of his thrombocytopenia?
- ((Ineffective production in the bone marrow::Megakaryocyte hyperplasia indicates increased platelet production, not ineffective production))
- ((Platelet destruction in the bone marrow::Platelets are not destroyed in the bone marrow))
- ((Platelet destruction in the liver::The liver is not the primary site of platelet destruction in cirrhosis))
- ((Platelet sequestration in the spleen::☑️ Portal hypertension causes congestive splenomegaly and hypersplenism, leading to increased platelet sequestration; bone marrow responds with megakaryocyte hyperplasia))
💡 The splenic vein normally drains into the portal vein, thus high portal venous pressure [from cirrhosis] transmits backwards into the spleen, causing increased congestive splenomegaly, expansion of the red pulp, and eventually fibrosis of the splenic trabeculae. Red pulp expansion in massive splenomegaly can sequester up to 90% of the body’s platelets. Bone marrow responds with megakaryocyte hyperplasia.