Stomach & Gastric Hormones
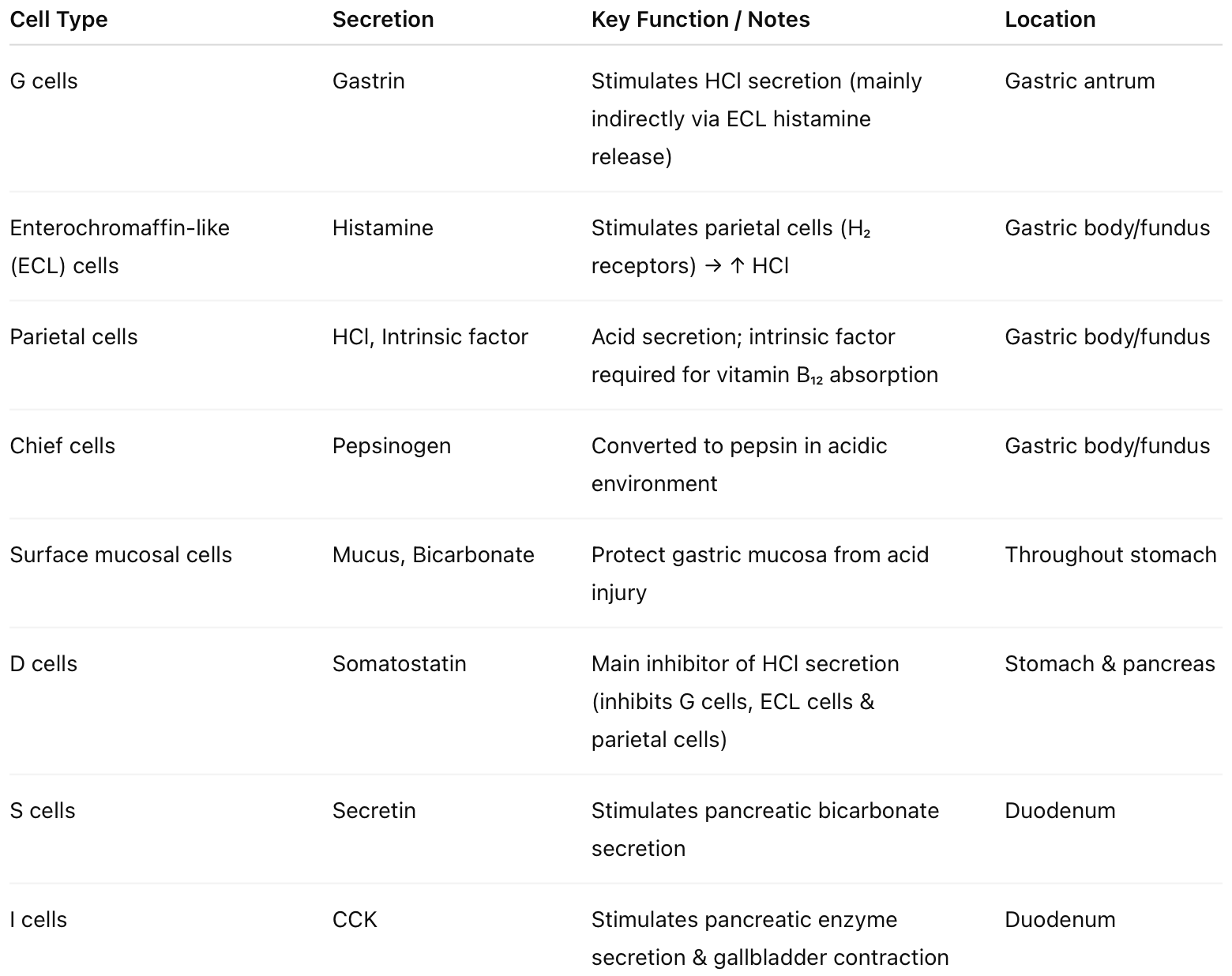
👩⚕️ Here's a summary table of the gastric hormones you need to know about! You should try drawing it - I'll attach my drawing below.
👩⚕️ Now work through these MCQs 😄
Which is true of gastrin?
- ((Increases gastric acid secretion::True, gastrin stimulates parietal cells indirectly via ECL cells, but this is not the most specific feature))
- ((Has a trophic effect on gastric mucosa::☑️ Stimulates growth of gastric mucosa and enterochromaffin-like (ECL) cells))
- ((Is mostly secreted from the gastric body::Secreted from G cells in the antrum))
- ((Increases secretion of bicarbonate from pancreas::Secretin stimulates pancreatic bicarbonate secretion))
- ((PPIs inhibit its production::PPIs increase gastrin due to loss of acid-mediated negative feedback))
Which cells does gastrin act upon to increase gastric acid secretion?
- ((Chief cells::Secrete pepsinogen, not hydrochloric acid))
- ((Brunner’s glands::Secrete alkaline mucus in the duodenum))
- ((Parietal cells::☑️ Note gastrin mainly increases acid indirectly (as well as directly) by stimulating ECL cells → Histamine → Parietal cells))
- ((D cells::Secrete somatostatin, which inhibits acid secretion))
💡Effects of gastrin
- Promotes hyperplasia and hypertrophy of gastric mucosa, especially in the body and fundus.
- Enhances stomach muscular contractions
- Binds CCKB-R on parietal cells → ↑ IP₃/DAG → ↑ Ca²⁺ → ↑ HCl and intrinsic factor secretion.
- Binds CCKB-R on ECL cells → secrete Histamine → binds H₂R on parietal cells → ↑ cAMP →↑ HCl
- The increase in acid production stimulates chief cells to increase pepsinogen secretion
Which of the following stimulates gastrin release?
- ((Adrenaline::Not a primary physiological stimulus for gastrin release))
- ((Glucagon::Does not stimulate gastrin secretion))
- ((Calcitonin::Not involved in gastrin regulation))
- ((Acetylcholine::☑️ Vagal stimulation releases acetylcholine (and GRP), which stimulates G cells to release gastrin))
💡 Stimulators of gastrin release:
- Gastric distension activates vagal stimulation and local relaxation
- Vagal stimulation acts on muscarinic receptors on G cells, via acetylcholine
- Amino acids in the stomach, e.g., phenylalanine
- Gastrin-releasing peptide, released from enteric nerves during the cephalic phase of digestion
Gastric acid secretion is due to a combination of which of the following?
- ((Gastrin, vagal stimulation, histamine::☑️ The three synergistic stimulators of parietal cells))
- ((Gastrin, vagal stimulation, secretin::Secretin inhibits gastric acid secretion))
- ((Gastrin, cholecystokinin, histamine::CCK is not a primary stimulant of acid secretion))
- ((Vagal stimulation, secretin, somatostatin::Secretin and somatostatin inhibit acid secretion))
💡 Stimulators of gastric acid release:
- Gastrin is released from G cells due to distension, vagal ACh, amino acids, GRP from enterics, and binds to
- CCKB-R on parietal cells → ↑IP₃/DAG → ↑Ca²⁺ → ↑HCl secretion
- CCKB-R on ECLs to stimulate the release of histamine
- Histamine binds to H₂ receptors on parietal cells → ↑cAMP →↑HCl secretion
- Vagal stimulation: Acetylcholine via M₃ receptor → Gq → ↑IP₃/DAG → ↑Ca²⁺ → ↑HCl secretion
Which intracellular messenger decreases gastric acid secretion from parietal cells?
- ((Calcium::Increases acid secretion via the IP₃ pathway))
- ((IP₃/DAG::Increases intracellular calcium and stimulates acid secretion))
- ((cAMP::☑️ Reduction in cAMP (via somatostatin, prostaglandins, noradrenaline) decreases H⁺/K⁺ ATPase activity))
- ((cGMP::Not a primary regulator of parietal cell acid secretion))
💡 ↑ cAMP → ↑ acid, ↓ cAMP → ↓ acid
Which of the following inhibits gastric acid secretion?
- ((Gastrin::Stimulates acid secretion via parietal and ECL cells))
- ((PGE₂::☑️ Binds EP₃ receptors on parietal cells, inhibits adenylyl cyclase → ↓ cAMP → ↓ acid secretion))
- ((NSAIDs::Reduce prostaglandin production, thereby increasing acid secretion))
- ((Vagal stimulation::Stimulates acid secretion via acetylcholine))
💡 Inhibitors of gastric acid release by direct action on parietal cells:
- Main inhibitor:
- Somatostatin → SSTR2, Gi → ↓cAMP → ↓HCl
- Prostaglandins (PGE₂, PGI₂) → EP₃ receptors → ↓cAMP → ↓HCl
- Noradrenaline via α₂ receptors → ↓cAMP → ↓HCl
- Secretin
- Others: Gastric inhibitory peptide (GIP), Vasoactive intestinal peptide (VIP), Glucagon
💡 Inhibitors of Gastrin release by direct action on G cells:
- Somatostatin inhibits G cells, ECL cells, and parietal cells - main inhibitor
- Prostaglandins (PGE₂): Direct inhibition and indirect via ↑ Somatostatin
- Low intraluminal pH, via D cell activation → ↑ Somatostatin
- Secretin
- CCK
- Others - Gastric inhibitory peptide (GIP), Vasoactive intestinal peptide (VIP), Glucagon-like peptide-1 (GLP-1), Calcitonin gene–related peptide (CGRP).
A woman suffers recurrent PUD despite PPIs and H pylori eradication therapy. Which of these is likely raised?
- ((Cholecystokinin::Stimulates pancreatic enzyme secretion, not associated with recurrent PUD))
- ((Histamine::Acts locally from ECL cells but is not typically elevated systemically))
- ((Secretin::Primarily stimulates pancreatic bicarbonate secretion))
- ((Gastrin::☑️ Recurrent PUD despite treatment suggests Zollinger–Ellison syndrome (gastrinoma) causing hypergastrinaemia))
Which hormone increases pancreatic secretion rich in bicarbonate?
- ((Secretin::☑️ Released from duodenal S cells in response to acidic chyme; stimulates pancreatic ductal bicarbonate secretion))
- ((Cholecystokinin::Stimulates pancreatic enzyme secretion, not bicarbonate-rich fluid))
- ((Histamine::Primarily stimulates gastric acid secretion))
- ((Serotonin::Not a regulator of pancreatic bicarbonate secretion))
💡 Effects of Secretin, released from S cells in duodenum in response to acid chyme and fatty acids:
- Secretin → SCTR → ↑ cAMP → Outcome depends on the target cell →
- Secretion of bicarbonate-rich pancreatic juice from pancreas ductal cells
- Stimulates bicarbonate-rich bile secretion through the bile duct’s cholangiocytes
- Trophic effect on pancreatic acinar cells
- Stimulates secretion of somatostatin from D cells
- Inhibits gastrin and gastric acid secretion
- Decreases gastric motility and delays gastric emptying to allow neutralization of chyme
- Enhances effects of CCK
💡 Effects of Cholecystokinin CCK, released from I cells in duodenum in response to fatty acids and amino acids in chyme:
- CCK → CCKB-R → ↑IP₃/DAG → ↑Ca2+ →
- Stimulates secretion of enzyme-rich pancreatic juice (lipase, amylase, proteases) from pancreas acinar cells
- Trophic effect on pancreatic acinar cells, promotes growth & maintenance of the exocrine pancreas
- Biliary: Stimulates gallbladder contraction and relaxes sphincter of Oddi allowing bile and pancreatic juice flow
- Delays gastric emptying to allow neutralisation of chyme
- Mild inhibition of gastric acid secretion
- Acts as a satiety signal, to decrease food intake (hypothalamic effect)
A patient has atrophic gastritis and presents with anaemia. Which anaemia is likely to be seen on a blood film?
- ((Macrocytic::☑️ Atrophic gastritis can cause pernicious anaemia due to intrinsic factor deficiency → vitamin B₁₂ deficiency → megaloblastic (macrocytic) anaemia))
- ((Microcytic::Seen in iron deficiency, thalassaemia, lead poisoning, sideroblastic anaemia))
- ((Spherocytes::Seen in hereditary spherocytosis or autoimmune haemolytic anaemia))
- ((Normocytic::Seen in anaemia of chronic disease or acute blood loss))
💡 Atrophic gastritis leads to loss of parietal cells, which produce intrinsic factors, essential for vitamin B12 absorption. Deficiency of B12 causes impaired DNA synthesis, resulting in macrocytic, megaloblastic anaemia, often with associated neurological symptoms such as glove-and-stocking paraesthesia, loss of vibration and proprioception, upper motor neurone signs, irritability.
Pernicious anemia is an autoimmune disease caused by antibodies against what?
- ((Erythrocytes::Not the primary mechanism in pernicious anaemia))
- ((Mucous cells::Not responsible for intrinsic factor production))
- ((Parietal cells::☑️ Autoimmune destruction of parietal cells → ↓ intrinsic factor → vitamin B₁₂ deficiency))
- ((Vitamin B₁₂::Deficiency occurs secondary to intrinsic factor loss, not direct antibodies to B₁₂))
A patient with pernicious anaemia taking IM vitamin B₁₂ 3-monthly presents with haematemesis and weight loss. Bloods reveal hypochromic microcytic anaemia. What is the diagnosis?
- ((Atrophic gastritis::Underlying condition in pernicious anaemia but does not explain haematemesis and weight loss))
- ((Gastric cancer::☑️ Pernicious anaemia increases risk of gastric adenocarcinoma; bleeding leads to iron deficiency (microcytic) anaemia))
- ((Duodenal ulcer::Would not typically cause weight loss and is less strongly associated with pernicious anaemia))
- ((Vitamin B₁₂ deficiency relapse::Would cause macrocytic, not microcytic, anaemia))
💡 A patient with pernicious anaemia is at increased risk of gastric cancer due to chronic atrophic gastritis, and new symptoms like haematemesis, weight loss, and microcytic anaemia suggest bleeding from a gastric malignancy.
In a patient with Ménétrier disease, what is the most likely finding?
- ((Hyperacidity::Acid production is reduced due to loss of parietal cells))
- ((Hypoalbuminaemia::☑️ Protein-losing gastropathy due to excessive mucus production leads to low serum albumin))
- ((Vitamin B12 deficiency::Not a typical feature))
- ((Hypergastrinaemia::Acid is reduced, but this is not the defining clinical finding))
In a patient with Ménétrier disease, which of the following is a recognised long‑term complication?
- ((Gastric adenocarcinoma::☑️ Increased risk due to chronic mucosal hypertrophy and hyperplasia))
- ((Iron deficiency anaemia::Can occur secondary to chronic mucosal bleeding))
- ((Peripheral oedema::Occurs secondary to protein loss and hypoalbuminaemia))
- ((Venous thromboembolism::Severe hypoalbuminaemia can predispose to hypercoagulability))
💡 Ménétrier disease is a rare hypertrophic gastropathy with massive enlargement of gastric rugal folds, protein-losing gastropathy, excess mucus production and decreased acid secretion. The thickened gastric mucosa leads to protein loss at the stomach, particularly albumin, resulting in hypoalbuminaemia and oedema due to low oncotic pressure.
A patient develops delayed gastric emptying following a gastrectomy. Which of the following is the most likely contributing factor?
- ((Increased cholecystokinin::Physiologically slows gastric emptying but not the typical post-surgical mechanism))
- ((Vagotomised::☑️ Loss of vagal (parasympathetic) stimulation reduces antral contractions and delays gastric emptying))
- ((Sympathetic loss::Would increase gut motility rather than delay it))
- ((Increased gastrin::Stimulates acid secretion, not gastric emptying))
💡 Vagotomy often accompanies gastrectomy and disrupts parasympathetic innervation, impairing gastric motility and leading to delayed emptying. This can cause bloating, nausea, and early satiety.
After gastric bariatric surgery, a patient develops sweating, palpitations, and convulsions. Diagnosis?
- ((Vagotomised early gastric relaxation::Not associated with hypoglycaemia or neuroglycopenic symptoms))
- ((Insulinoma::Unlikely in the immediate post-bariatric setting))
- ((Dumping syndrome::☑️ Rapid gastric emptying causes hyperinsulinaemia leading to hypoglycaemia with adrenergic and neuroglycopenic symptoms))
- ((Pheochromocytoma::Would cause palpitations and sweating but not post-prandial hypoglycaemia))
💡 Early vs Late dumping syndrome
- Early dumping syndrome
- Occurs 15 to 30 minutes after eating
- Post-operative loss of pyloric regulation causes hyperosmolar, sugar-rich foods move too quickly from the stomach into the small intestine
- The intestinal lumen is highly hyperosmotic relative to the plasma hence the concentrated chyme entering the small intestine triggers dramatic osmotic shifts: the fluid moves rapidly from the plasma into the intestinal lumen causing intestinal distension, hypovolemia, abdominal pain, bloating, diarrhea, hypotension, tachycardia, dizziness
- Rapid chyme stimulates release of enterogastrones (secretin, CCK, GIP, GLP-1) which slow gastric emptying and stimulate pancreatic & biliary secretions
- Late dumping syndrome
- Occurs 1 to 3 hours after eating
- The rapid absorption of sugars from the chyme triggers the pancreas to release a large surge of insulin
- The excessive insulin causes reactive hypoglycaemia and symptoms of sweating, tremor, anxiety, fatigue, and confusion
- Management: Eat smaller, more frequent meals, limit high-sugar foods, acarbose or octreotide may slow gastric emptying, surgery may be needed
In a posterior gastric perforation, where does the fluid collect first?
- ((Hepatorenal (Morrison’s) pouch::Fluid may collect here later in supine patients but not initially in posterior perforation))
- ((Greater sac::Anterior gastric perforations spill directly into the greater sac))
- ((Omental bursa::☑️ In a posterior gastric perforation, gastric contents enter the lesser sac (omental bursa = lesser sac) first))
- ((Pelvic cavity (rectovesical/rectouterine pouch)::Dependent collection site but not the first site in posterior gastric perforation))
💡 In a posterior gastric perforation, gastric contents enter the lesser sac (omental bursa = lesser sac) first. Fluid may later spread to the greater sac via the foramen of Winslow.
In an anterior gastric perforation, gastric contents enter the greater sac of the peritoneal cavity. This results in widespread peritonitis and pneumoperitoneum.